South Australian Medical Heritage Society Inc
Website for the Virtual Museum
Home
Coming meetings
Past meetings
About the Society
Main Galleries
Medicine
Surgery
Anaesthesia
X-rays
Hospitals,other organisations
Individuals of note
Small Galleries
Ethnic medicine
- Aboriginal
- Chinese
- Mediterran
Kuru
ACKNOWLEDGEMENT
We are most grateful to Dr. Anthony Radford who kindly allowed us to include his
PowerPoint presentation among the Internet series of Talks given to the Society by
its members and invited speakers.
Dr Radford first visited New Guinea (then TPNG) in 1959 as a senior medical student and
later returned to establish a successful rural medical practice. He recorded fifty
years of his experiences in a book called "Singsings, Sutures and Sorcery".
He was one of the many South Australians who contributed to the advances in public health
in the area. His experience with the solving of the Kuru mystery is revealed in paper
which he and Dr. Roy Scragg published in November 2013 entitled
"Discovery of Kuru Revisited: How Anthropology Hindered Then Enhanced Kuru Research".
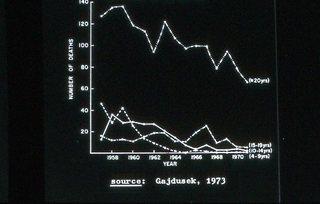
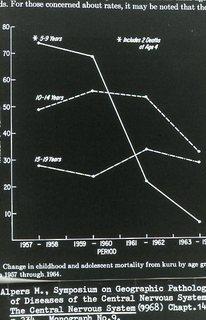
His slides deal with the early theories and the possible causes of Kuru, an incurable transmissible spongiform encephalopathy, formerly endemic in the Fore tribe of the Okapa District, Papua New Guinea. In his talk he mentioned Daniel Carlton Gajdusek, who used monkeys to confirm the transmission of the disease, and drew parallels with Creutzfeldt-Jakob Disease, and prions as a possible causal protein. In 1976, Gajdusek was a co-recipient of the Nobel Prize in Physiology or Medicine for his work on kuru, along with Baruch Samuel Blumberg (for his research on Hepatitis B).
Who first described the signs and symptoms of kuru?
&
the role of social science in the elucidation of its aetiology?
Anthony J Radford
23 May 2013
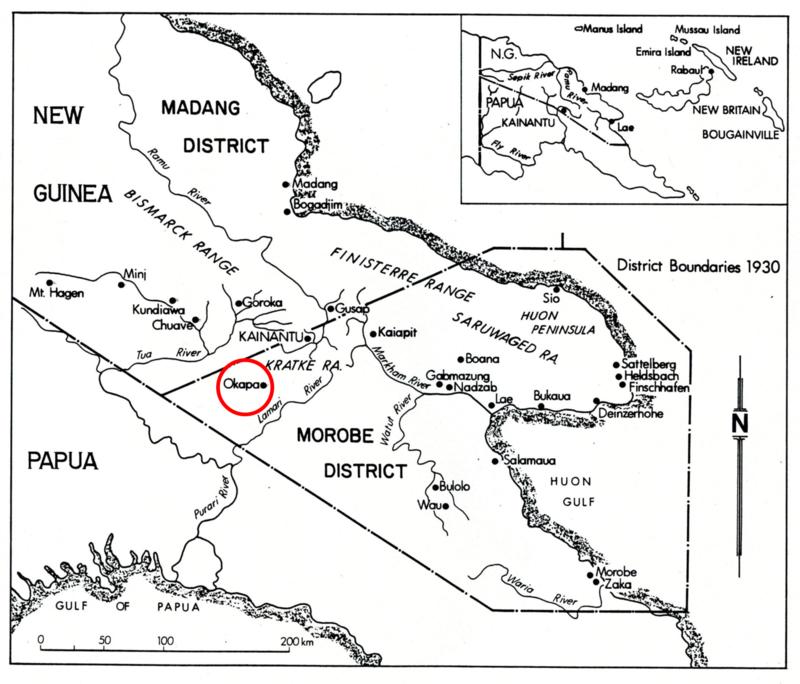
Table 1: New Guinea has had many sentinel medical world highlights:
- Enteritis necroticans (Clostridium perfringens) by Tim Murrell
- Iodised oil to prevent goitre and endemic cretinism by McCullagh, Pharoah and Hetzel
- Use of tetanus toxoid in pregnant women to prevent neonatal tetanus by Frank Schofield
- Use of pneumococcal vaccine by Douglas and Riley
* Murrell, Hetzel, Douglas were all from Adelaide.
... and then there is KURU.

Photo AJR.
Table 2: Kuru signs and symptoms
- Initially the patient noticed mild intermittent unsteadiness when crossing a narrow bridge into a garden.
- Instability then increased, followed by tremors and, finally, quite violent shaking developed.
- Eventually the patient was unable to walk, and then even to stand.
- The victims became totally dependent on their care by others.
- They developed facial grimaces. Some developed emotional lability.
- At the end they were unable to swallow and progressive emaciation occurred.
- Finally, intercurrent infection – usually pneumonia, and large decubitus ulcers developed which caused immense distress to both victims and relatives.
- In a few the infection extended into the medulla of the brain, up into the areas controlling breathing and death occurred from respiratory failure.
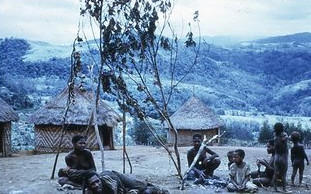
Photo AJR.
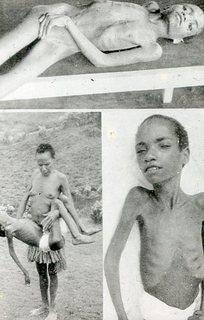

Photo AJR.
This paper:
- describes the sequence of events which led to the earliest descriptions of kuru, and
- the role of social science,
- first in delaying any medical assessment and investigation due to a belief of a sorcery origin, and
- then in the development of the theory that its transmission was related to cannibalism,
- illustrating the value of multidisciplinary approaches to many epidemiological problems.
Diseases which don’t fit into standard medical reference are often ascribed:
- to sorcery or the supernatural in the animist world, or
- to a psychosomatic origin in our own; such as epilepsy, gastric ulcers, and
- Unexplained community infertility in more primitive communities, including New Guinea, also fall into this group as Roy Scragg has shown ...
- ... AND so did KURU.
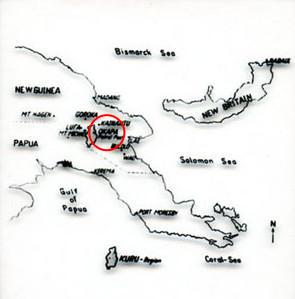
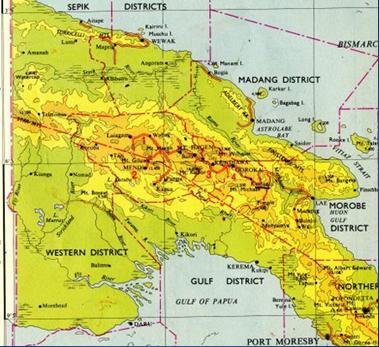

Photo AJR.


Photo AJR.

Photo AJR.

Courtesy Bill Brown.
South Australian 'Honour Board'
The Adelaide Group:
- Professor Norrie Robson (physician)
- Professor Henry Bennett (geneticist)
- Mr Donald Simpson (neurosurgeon)
- Dr Harry Lander (physician)
- Dr Clive Auricht, Dr Bronte Gabb & Caroline Leach
- Dr Michael Alpers
- Dr Roy Scragg
| Table 3: Earliest references & descriptions. | |
|---|---|
| Arthur T. Carey | 1950-51 |
| Ronald & Catherine Berndt | 1951 in Berndt R, 1958 |
| John R. McArthur | ? Dec 1953 (in Z & G 1957) |
| William 'Bill' Brown | February 1954 |
| John R. McArthur | August 1954, 1955 |
| John Colman | September 1956 |
| Frank Earl | September 1956 |
| Vin Zigas | December 1956 |
| Charles Julius | January 1957 |
| Roy Scragg | February 1957 |
| D. Carleton Gajdusek and Vin Zigas | November 1957 |
| Vin Zigas and D. C. Gajdusek | November 1957 |
It was government patrol officers who, three to five years earlier, were the first to report and describe the features of 'kuru' .
"one of the vast group of chronic, progressive, heredo-familial degenerations of
the central nervous systems ... though genetic predisposition is strongly suggested ... but
any ethnic environmental variables [operating] ... have not been determined."
(Zigas and Gajdusek, 1957).
| Table 4: Postulated causes of Kuru | ||
|---|---|---|
| Sorcery | Fore villagers | Decades |
| Psychosomatic | Patrol officers & R. Berndt | 1950s |
| Encephalitis with post-encephalic signs | H. F. Earl | 1955 |
| Hysteria | Vin Zigas | 1955 |
| Somatic illness: type unknown | C. Julius | 1956 |
| Chronic progressive heredo-familial encephalopathy | C. Gajdusek & V. Zigas | 1957 |
| Toxic - 'Strongly suggested' | R. Scragg; D. C. Gajdusek & V. Zigas | 1957 |
| Genetic polymorphism | J. H. Bennett et al. | 1957 |
| Slow virus with very long incubation | W. Hadlow | 1959 |
| Prion | S. Pruisner | 1982 |