South Australian Medical Heritage Society Inc
Website for the Virtual Museum
Home
Coming meetings
Past meetings
About the Society
Main Galleries
Medicine
Surgery
Anaesthesia
X-rays
Hospitals,other organisations
Individuals of note
Small Galleries
Ethnic medicine
- Aboriginal
- Chinese
- Mediterran
The discovery of amoebic meningitis in Northern Spencer Gulf towns
ACKNOWLEDGMENT: We are grateful to Dr. .Robert B. Cooter A.M. and Dr. Rodney F. Carter for the details and chronology of the discovery, an example of co-operation between a country general practitioner and a city medical scientist..

The north of Spencer Gulf viewed from Port Augusta. Flinders Ranges and Transcontinental railway bridge in background. Mangroves on beach.
Between 1947 when a water pipeline from Morgan to supply towns of the Northern Spencer Gulf was completed and 1972 there were 20 documented fatal cases of Meningitis mainly in children and young adults. Many of these were proven to be caused by a type of amoeba which often results in a fatal meningitis.
The casual organism is found in soil and tepid water. It enters the brain through the olfactory epithelium while swimming, diving or nasal douching. The infection has a high mortality rate and after the South Australian discovery cases have been reported from the USA , Czech Republic and elsewhere.
Drs. Fowler and Carter were pathologists at the then Adelaide Children’s Hospital while Dr. Cooter was a general practitioner in Port Augusta who referred his patients to the Children’s Hospital and had a keen interest in the disease.
The identification of the Amoebic nature of the meningitis was made by Dr. Malcolm Fowler and Dr. Rod Carter who studied autopsy brains from four cases of the meningitis from the area in 1965. The amoeba bears Dr. Fowler’s name “Naegleria fowleri”. They reported their findings in medical journals as well as to Dr. Cooter who commenced to examine the cerebrospinal fluid of his patients using the high power of his microscope. He described his findings in a further patient in a referral letter in 1966 and was thus the first clinician to make a bedside diagnosis of amoebic meningitis from his own microscopic examination of the patient’s CSF.
The following material was added at the request of Dr. Cooter in December 2008:
"... by detecting the living amoeba when we were viewing the spinal fluid of the 1966 victim (a 10 yr old boy) under high power microscopy, for the first time in Australia , and probably in the world".
Later, when researchers were unable to find the source of the infection, Dr. Cooter and Dr. Mickan researched environmental (water temperature, etc.) and epidemiological factors including the case histories of the young fatal victims with their ablution habits. These habits involved entrance of the water into the nasal cavities, such as .
Forcing tap water up the nostrils to clear a sinus problem.
Squirting water up the nose from a hose to remove salt water after swimming in the Spencer gulf .
Snorkelling in the bath.
These ablution habits aroused the suspicions of Dr. Cooter and Dr. Mickan that the amoeba originated in the pipeline water in the summertime with a temperature range (35-45c) favourable to the multiplication and increased pathogenicity of the amoeba." "Then a letter from Dr. Cooter was sent to the Eng.&WS Dept. and then he interviewed Dr. Kevin Anderson, and expressed his suspicions and concerns about the pipeline water. Dr. Anderson then discovered the amoeba in the water supply to one of the victim's home." "Thus, 2 of the 3 crucial findings in the discovery of the disease have been attributed to two general practitioners in Port Augusta.
- The discovery and identification of the living amoeba
- Directing Dr. Anderson to its source based on our local research as described.
The amoebic meningitis findings contributed to our rich experience as rural GPs and was mentioned in context with a distinguished alumni award [I received] for services to rural medicine and the Florey chapter of the alumni association from Adelaide University bestowed on me at the Commemoration ceremony 18/12/2008....."
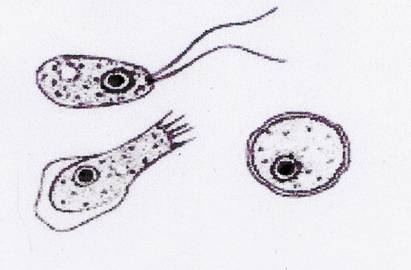
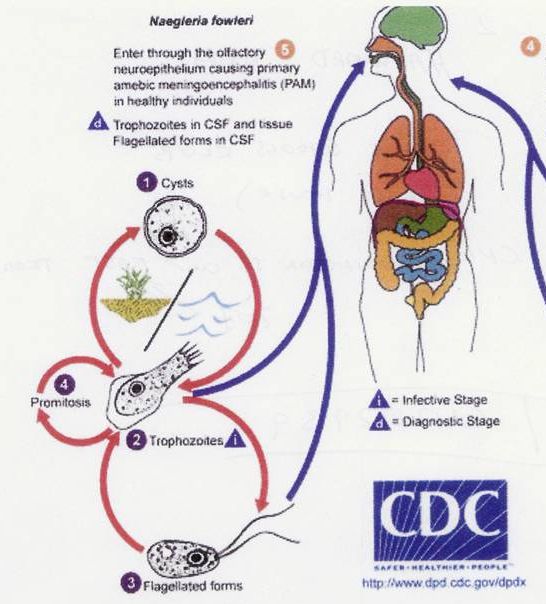
Illustration from Wikipedia showing Naegleria fowleri as a cyst (right) and flagellate and trophozoite forms (upper and lower left). The latter are infective and enter the brain through the olfactory neuro-epithelium.
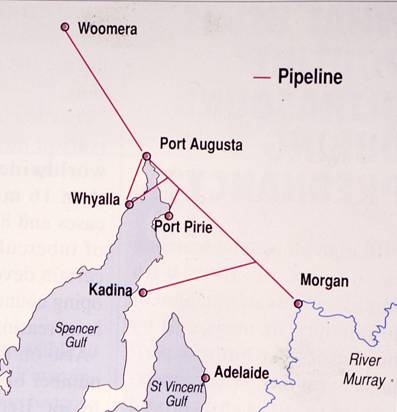
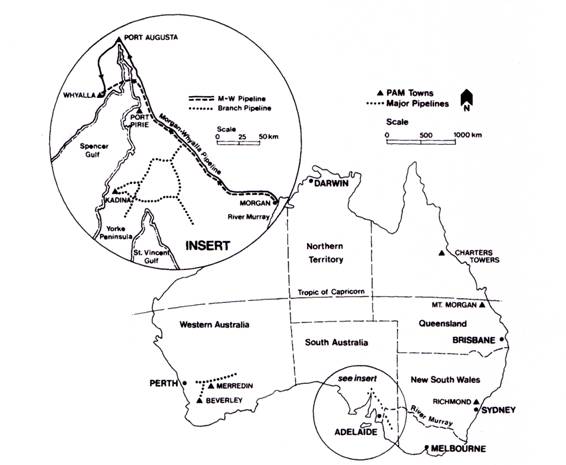
Map showing the Morgan to Upper Spencer Gulf Pipelines
.
The incidence of meningitis was: Port Augusta 15, Port Pirie 3, and Kadina 2. Drs Cooter and Mickan postulated that Woomera and Whyalla were spared because the water temperature in the exposed pipes exceeded 45 0c. The lower water temperatures, 35 0 to 40 0 allowed the cysts to change into flagellate forms which are infective.
Amoebae were found later in the water supply (household tap) by Dr. Anderson. This was carried out in summer as attempts in winter failed due to low water temperature.
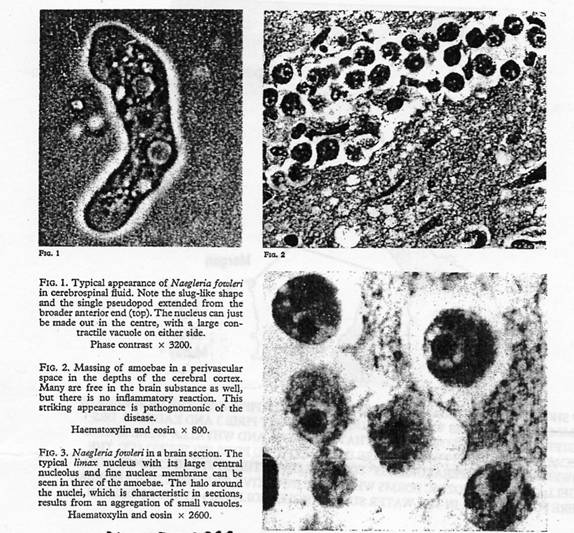
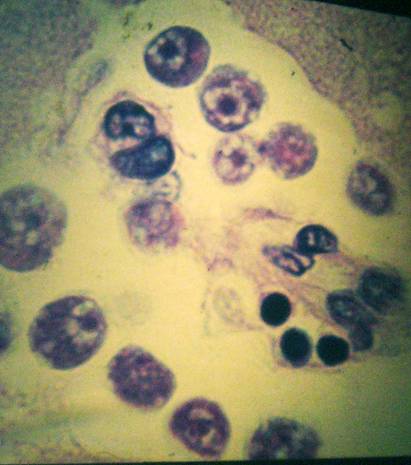
The following colour photographs from the Pathology Department from the Adelaide Children’s Hospital have been kindly loaned to Dr. Cooter by Dr. Carter.
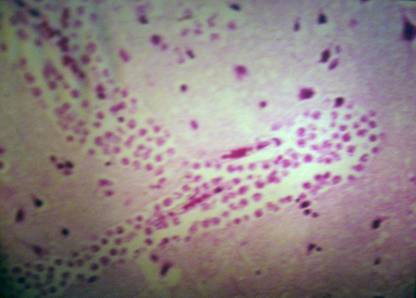
H & E STAIN of perivascular space (Fig2).

References:
Cooter R. Australian Family Physician. 2002 31, 4, 399-400
Cooter R. The Life of a Doctor with Missions in Rural Medicine” : Railmac Publications, Appendix 2, 78-86.
Carter R.F. 1972 Primary amoebic meningo-encephalitis. An appraisal of present knowledge. Trans Soc Trop Med Hyg. 66(2): 193-213.
Carter R.F.1968 Primary amoebic meningo-encephalitis: clinical pathological and epidemiological features of six fatal cases.J. Pathol Bacteriol. July 96(1):
Fowler M. & Carter RF.1965 Acute pyogenic meningitis probably due to Acanthamoeba sp: A preliminary report. Br. Med. J. September 25, 2 (5464): 740
APPENDIX:
Additional information about chlorination of water-supply and occurrence of other meningitis cases in Australia has been kindly provided by Dr. Bret Robinson, Senior Protozoologist at the Australian Water Quality Centre at Bolivar South Australia . The relevant map, references and comments are outlined below.
 The map from Ref: 1 showing the towns with PAME (primary amoebic meningo-encephalitis) infections.(1955-1981) and their associated water pipelines of significance.
The map from Ref: 1 showing the towns with PAME (primary amoebic meningo-encephalitis) infections.(1955-1981) and their associated water pipelines of significance.
Additional references
1. Dorsch MM, Cameron AS, Robinson B: (1983) The epidemiology and control of primary amoebic Meningoencephalitis with particular reference to South Australia . Trans Soc Trop Med Hyg, 77,.3, 372-377 :
2. Robinson, B S (1977), Effectiveness of chlorine in the control of Naegleria: laboratory and field studies in South Australia . Proc. 7th. Federal Convention Australian Water and Wastewater Association, Canberra 1977 pp 465-478.
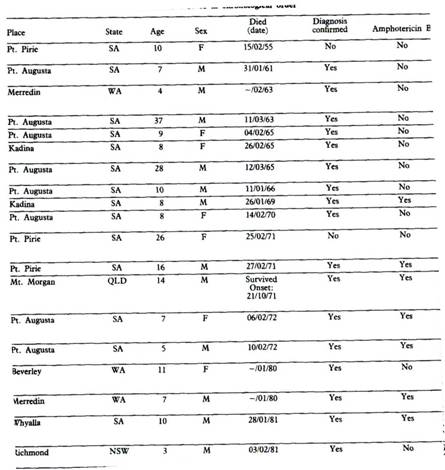
The map insert outlines the additional confirmed cases of Naegleria Meningo-encephalitis in Australia between 1955 and 1981. There were no further cases in the Spencer Gulf area after 1972 presumably due to attention to chlorination of the water pipe line but also and mainly due to chlorine in the local supply..
Ten years later (1980 –1982) several additional cases were reported. Whyalla in 1981. Other reports arrived from towns in NSW, Queensland and WA.: (Richmond NSW.1981,Merredin WA. 1982, Beverley and York WA. 1980,.and Charters Towers QLD 1982)..The sporadic nature was suggestive of local rather than general factors. These are summarised in the table below from Ref:1. There was one additional case in 1995 when an American couple camped at Branch Creek and swam in the billabong. The husband died in Darwin . (personal reference Bret Robinson)
The conclusions reached by the authors of the above publications seem to indicate that while there are some doubts about the effectiveness of chlorination by some researchers, it appears that chlorine concentrations of 0.5mgms per litre of local water supply make the risk of PAME infection negligible.(Ref. 1)
The length of the pipeline and the difficulty of maintaining effective concentrations over long distances was noted during the Spencer Gulf outbreak and additional chlorination stations were added to the pipe line. A more stable form of chlorine in the form mono-chloramine NH2Cl also improved the degree of disinfection. Attention to local chlorination was vital.
The authors also suggested that air transmission by air-borne dust is unlikely as cysts of Nagleria fowleri will be desiccated within five minutes
The authors briefly refer to the relative ineffectiveness of antibiotics such as Amphotrricin B, Miconazole, Rifampicin and others. There has been little change but combinations such as Floconozole, Amphotericin B, Rifampicin and Azithrumacin have been recently reported to be of some use. (source: pubmed)
The scattered and diffuse incidence of the disease in Australia during 1980-1982 is difficult to explain. The disease occurs almost invariably in the summer months, but while Merredin and Beverley (WA) lie on the Kalgoorlie pipeline the NSW. and Qld. cases were associated mainly with local swimming pools. It may be possible that as in the Czech Republic the source could have been in an isolated side pool which escaped general chlorination. .Dr. Robinson suggested another possibility. The diffuse incidence may be related to the generally low densities of the amoebae in water with insufficient dose of inoculum required for infection. However in some areas, due to lack of chlorination or other factors such as temperature, soil contamination and stagnation. the inoculum will be large enough to be infective.
A French group studied the incidence and numbers of amoebae associated with nuclear reactor cooling systems. It has developed a risk analysis model which predicts the likely incidence of PAME as a function of the degree of contamination. Based on their animal work the French Health Authorities have set a maximum level of 100 N. fowleri per litre not to be exceeded in watercourses where human exposure is possible.
Reference.:
Applied and Experimental Microbiology, July 2001, p.2927-2031.
-o0o-