South Australian Medical Heritage Society Inc
Website for the Virtual Museum
Home
Coming meetings
Past meetings
About the Society
Main Galleries
Medicine
Surgery
Anaesthesia
X-rays
Hospitals,other organisations
Individuals of note
Small Galleries
Ethnic medicine
- Aboriginal
- Chinese
- Mediterran
Early Rigid Endoscopes
ACKNOWLEDGEMENTS: We are most grateful to Sister Carol Saniotis Director of theatre nurses at TQEH, Jan Hooper OAM, chairman of the QEH historical society and Margo Waye the archivist at RAH history museum for allowing us access to their heritage items.
The insertion of a metal tube into the colon or bladder is an easy procedure, but observing the contents is difficult without good illumination. If the inner diameter of the tube is less than one centimetre, then the light bulb must smaller. Such globes became available at the turn of the 20th century, and enabled visualisation of almost all hollow organs.
The ability to shine a light from the end of a sigmoidoscope or procto-scope, and perhaps advance a biopsy forceps to obtain a tissue sample for diagnosis, was a welcome advance.
SIGMOIDOSCOPY

Three sigmoidoscopes of various lengths and diameters, the obturators (plugs with ring handles) for easy insertion are inside, and light source is at top left.
Once the sigmoidoscope is inserted, the obturator is withdrawn, and light source is attached.


The sigmoidoscope almost fully assembled. The insufflator is used to dilate the bowel, and the power for the light source is next to it. The viewing is excellent, and one can introduce biopsy forceps to obtain a sample for diagnosis.
GASTROSCOPY
Viewing of the entire stomach was not possible before the arrival of fibre-optic endoscopy. The upper part of the stomach could not be seen, but the duodenum and distal stomach could be seen, and biopsies could be taken.
-
 An early gastroscope.
An early gastroscope. -
 A flexed gastroscope.
A flexed gastroscope.


Once in the stomach, the end of the scope could be bent to about 30 degrees, but not more, by twisting round the small wheels distal to the eyepiece. Thus the upper stomach and the fundus could not be seen. Fibre-optics allowed a “J-manoeuvre”, in which the end of the scope points backwards, and the fundus and entry of the oesophagus can be seen.


HYSTEROSCOPE
The hysteroscope has been developed to enable to see the inside of the womb for diagnostic purposes, and to monitor the effect of treatment. A novel idea was the development of a cover for the eyepiece which could be connected to visual display unit and provide a real-time picture.
-
 An standard hysteroscope.
An standard hysteroscope. -
 Hysteroscope and eyepiece cover.
Hysteroscope and eyepiece cover.


The photo on the right shows the eyepiece cover and a connection for the VDU. A great advance for recording and documentation.
Cystoscopes
There were other long and short "tubes" to visualise the gullet, ears, and nasal passages, but cystoscopes were important to visualise the urinary bladder.

A basic cystoscope. The end is slightly curved to pass the prostate gland, and the taps at the end allow water to flow in and out. Once inserted, urine is drained out and replaced by water or saline. Some of the air which has remained in the bladder forms a bubble at the top centre of the bladder, which becomes a reference point for orientation.

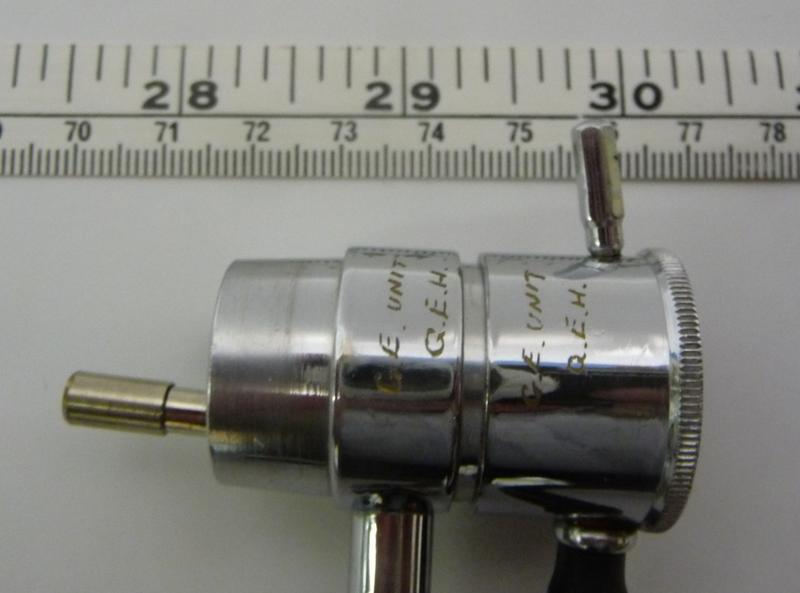
The proximal end of a cystoscope showing the eyepiece, an irrigation channel in the centre, and two entry points for ureteric catheters to pass up the ureters to visualise the kidneys. The knurled knob on the right raises or lowers the Albarran lever.
-
 Albarran lever down.
Albarran lever down. -
 Albarran lever up.
Albarran lever up.


Lifting the Albarran lever will bend the ureteric catheter and make it easier to canulate the ureter. After injection of the contrast the kidney is seen.
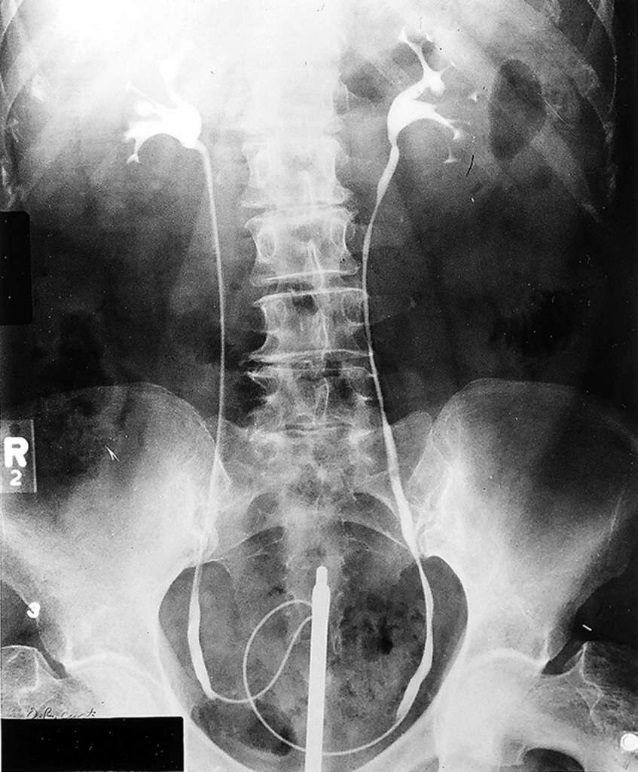
A retrograde pyelogram showing a cystoscope in the bladder, ureteric catheters coiled up in the bladder and passing up the ureters, ending at brim of the pelvis. The Xray shows the kidneys and the collecting systems.
Trans-Urethral Resection of the Prostate (TURP)
One of the major advances in urology was the development of the trans-urethral resection of the prostate (TURP). Previously, the enlarged prostate adenoma was enucleated digitally through an abdominal incision.
Bleeding and incontinence were some of the early complications. In the period between the two World Wars, many trans-urethral approaches were developed to remove small portions of the prostate (5x5mm) using coagulation or high frequency current.

An early resectoscope showing the cystoscope component. Please note the brown insulating sheaths used to protect the urethra from heat injury. A black lever (in the right end of the box, just under the lower insulating sheath) used to advance the resecting loop, is assembled.

Because of the small samples obtained, the time for adequate resection varied between one to 2-3 hours.
Appendix
A very brief overview of the history of endoscopes.
| c. 600 BCE | Early primitive otoscope mentioned in the Shushruta-Samhita. |
| c. 9th C CE | Abu-al-Qasim (aka Abucasis) invents devices to inspect internal cavities. |
| 1743 | Andre Levret creates a speculum with an artificial light source. |
| 1780 | Samuel Vogel first visualised the ear drum of a living patient. |
| 1808 | Philip Bozzini creates the "lichtleiter" ("light conductor") , the first modern endoscope. |
| c. 1860's | Further improvements to light source and lenses by Antonin Jean Desormeaux, Francis Cruise, Alfred Couriard, etc. |
| 1866 | A water cooled, distal incandescent platinum light source was devised by Julius Bruck. |
| 1877 | Maximilian Nitze greatly improved the Field of View, added microscope optics. |
| 1880 | Edison's light globe was released. |
| 1883 | David Newman creates the first urethroscope with a distal electric bulb. |
| 1886 | Nitze adds forceps with electro-cautery tips to his endoscopes. |
| c. 1901-1910 | Georg Kelling performs the first laparoscopy on a living person. Beginning of the modern techniques. |
| 1908 | Ringleb added new optics, increasing Field of View, brightness, magnification. Used until the 60's. |
| 1932 | A semi-flexible gastroscope with 48 lenses is created by Rudulf Schindler. |
| 1957 | Basil Hirschowitz and Larry Curtiss created the first fibre-optic endoscope. |
| 1961 | First commercially available fibre-optic gastroscope, the "ACMI 4990 Hirschowitz fiberscope". |