South Australian Medical Heritage Society Inc
Website for the Virtual Museum
Home
Coming meetings
Past meetings
About the Society
Main Galleries
Medicine
Surgery
Anaesthesia
X-rays
Hospitals,other organisations
Individuals of note
Small Galleries
Ethnic medicine
- Aboriginal
- Chinese
- Mediterran
Obstetric forceps, then and now
ACKNOWLEDGEMENTS
We are most grateful to Jessica Tyndall, the Medical Librarian who manages the Gus Fraenkel library at the Flinders Medical Centre. Ms Tyndall provided us with strong encouragement, stimulated us and gave her permission to photograph the Emeritus Professor Warren Jones' collection of obstetric forceps stored in the Fraenkel library. Professor Jones and Dr Christopher Verco also provided much relevant background information and comments. We also thank Dr. Colin Suchting, a retired obstetrician and gynaecologist, who provided his own pair of forceps and kindly loaned us the book by Leonard E. Laufe about the forceps history and use. Professor Donald Simpson as always was most supportive and helpful.
Before the 15th century, difficult and obstructed childbirth often endangered the life of both mother and child. The solution then was to use destructive instruments to decrease the size of the of the stillborn child, in order to save the mother's life. References to such procedures are found in the early Indian literature and in the writings of Hippocrates. There were some references of early manual traction or the use of mesh wrapped around the foetal head, but the success rate was minimal and probably resulted in mutilation of the head.
A possible early forceps used by Jacob Rueff in Zurich in 1550's are shown on the left. It is unlikely that they could be separated and therefore were likely to mutilate the head. On the right are the Chamberlen forceps. They were inserted separately and then tied or "locked" together. The Chamberlen families were the noted accoucheurs to the English Royal Houses (1600-1728)
The Chamberlens, a French medical family, arrived in England from Paris in 1569 because of religious persecution. Their son Peter was born in 1572, and it is likely that he was the inventor of the forceps. The family continued in their obstetric tradition and kept their invention secret for almost one hundred years. Peter M Dunn (Arch Dis Child Fetal Neonatal Ed 1999; 81: F232-F235) describes how they arrived at the "expecting household" with a large ornate box, blindfolded the mother, and forbade anyone to enter the lying-in room. The relatives gathered outside heard bells and other strange noises accompanying the delivery.
No secret could be kept forever. After the middle of the 18th century, numerous variations of the Chamberlen apparatus were produced by Palfyn, Dusee, Giffard, Smellie, Simpson, Tarniere, Kielland and others ( Obstetric Forceps, Leonard E Laufe, Harper and Low 1968).
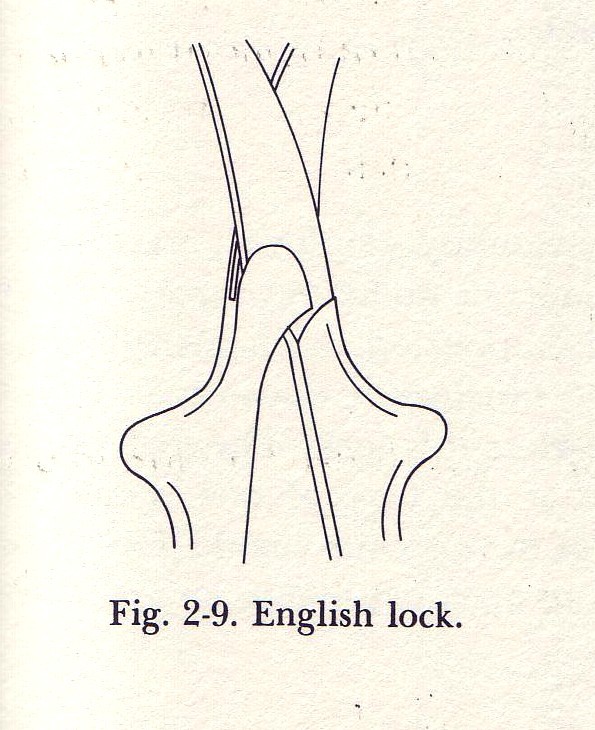
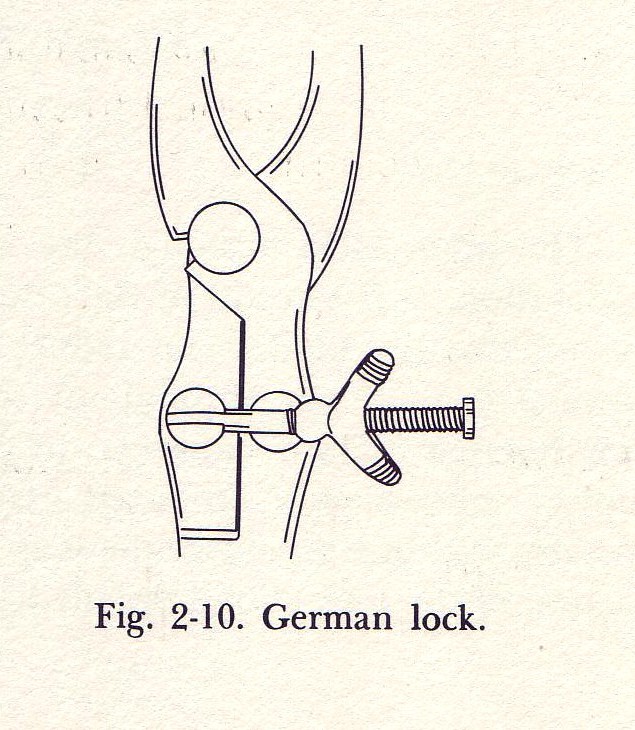
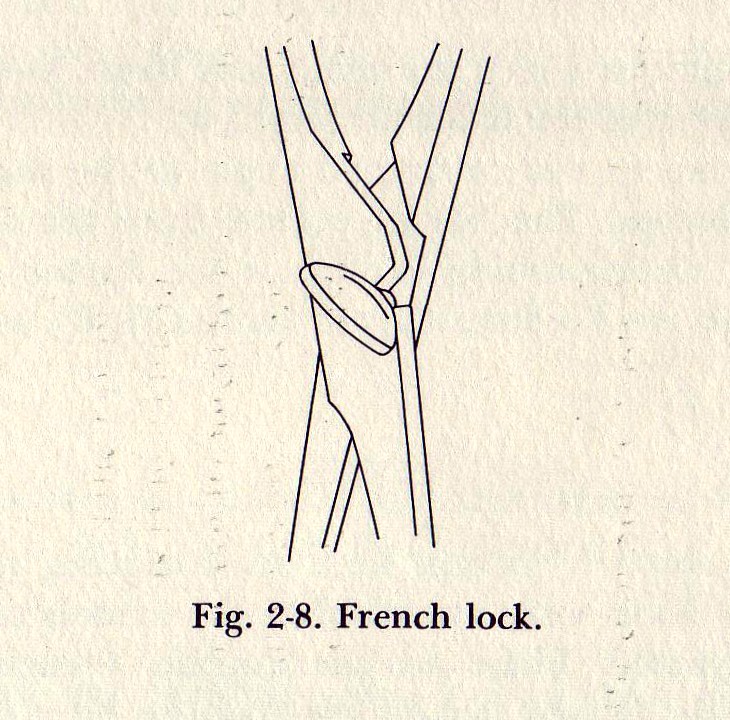
The common procedure was the insertion of the individual forceps separately and then joining them around the foetal head using a locking device. The variety of these devices, including French, German and English locks, indicate the plethora of such variations and the inventiveness of their producers. The main aims of the forceps are to provide the ability to exert traction, and to enable rotation of the head. There is some inevitable degree of compression to prevent slippage of the blades, but this is minimal in skilled hands. The degree of compression has been measured using strain gauges, and is usually less than 6 lbs/sq inch. Finally the forceps have an additional function, which is to partially dilate the birth canal. Professor Simpson commented that difficult forceps delivery sometimes resulted in in intracranial bleeding from tearing a vein at the rigid junction of the falx and tentorium. This was occasionally seen in Adelaide as late as the 1950's.
The blades have two curves. The cephalic one surrounds the foetal head. A pelvic curve follows the contour of the pelvis. Several models have an added traction device designed to follow the pelvic curve more easily. In the beginning of their use their application was classified as High (above the pelvic floor), Middle and Low (usually when the foetal head is on view). Today the first two are no longer used, and are considered to be dangerous. A Caesarean section is now usually performed instead. While the use of forceps in obstructed labour was common in the early half of the last century, their application is now rare.
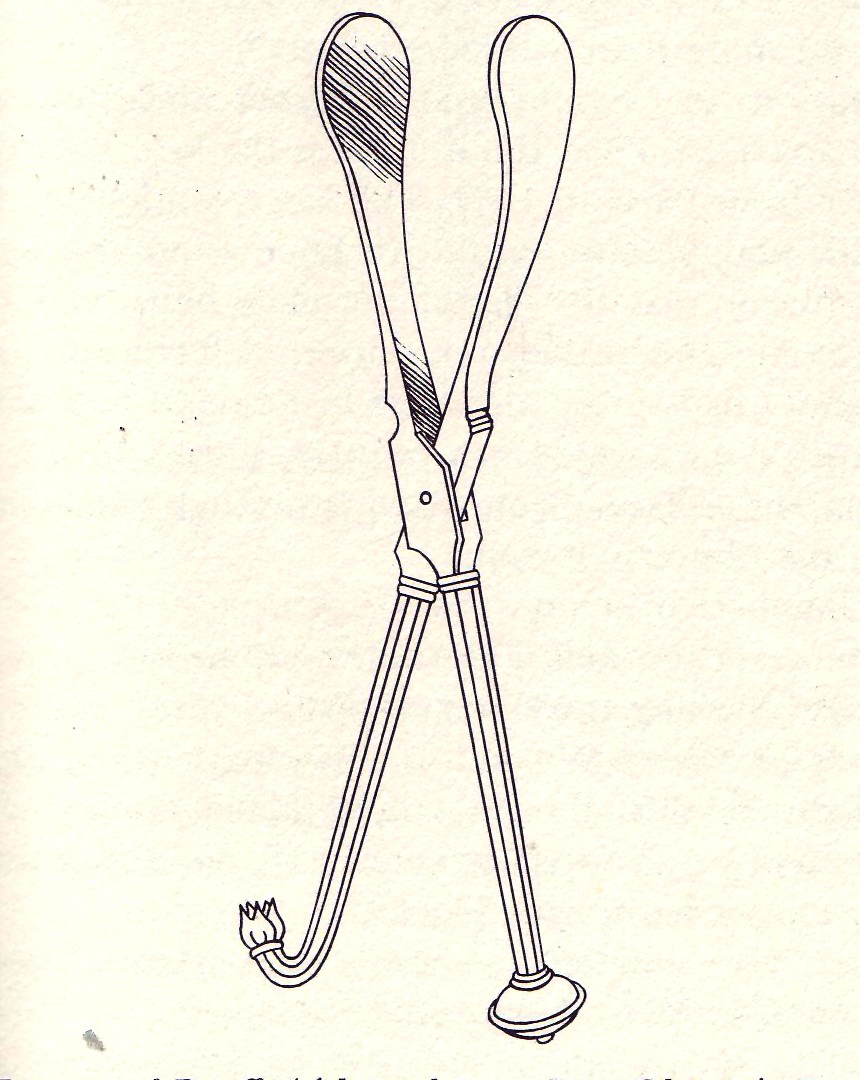
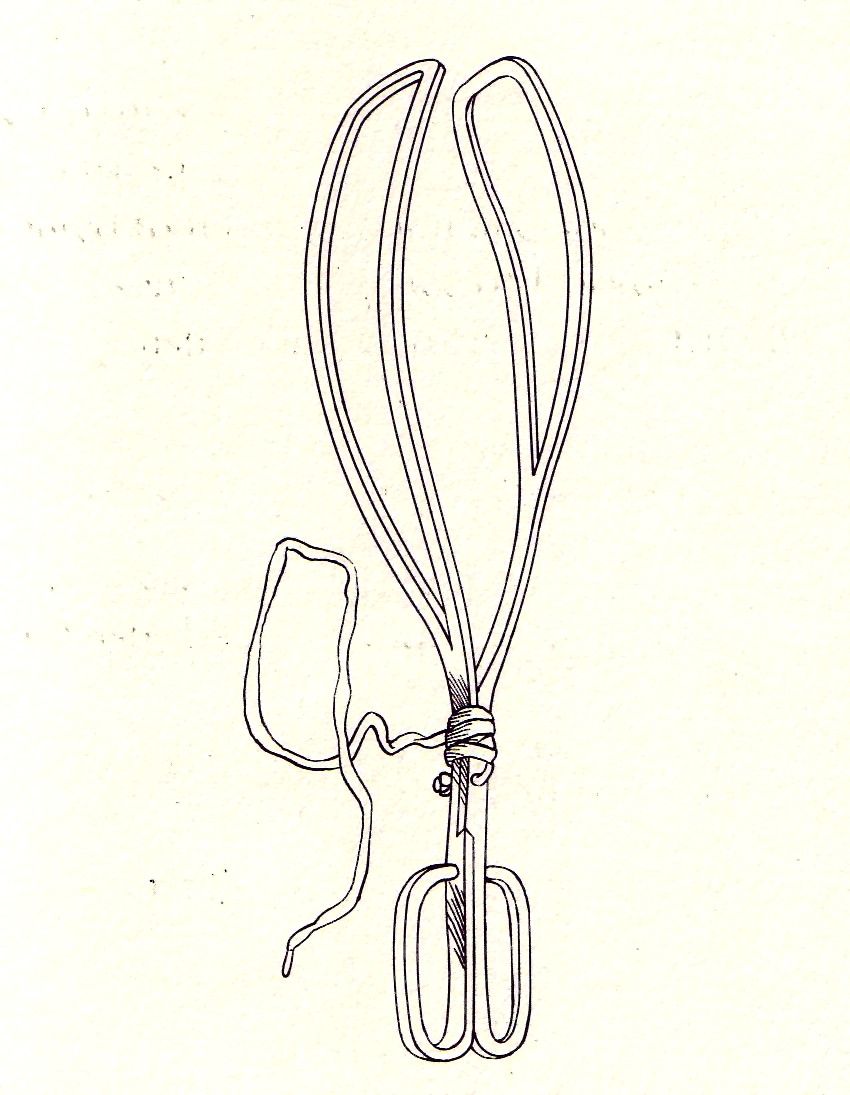
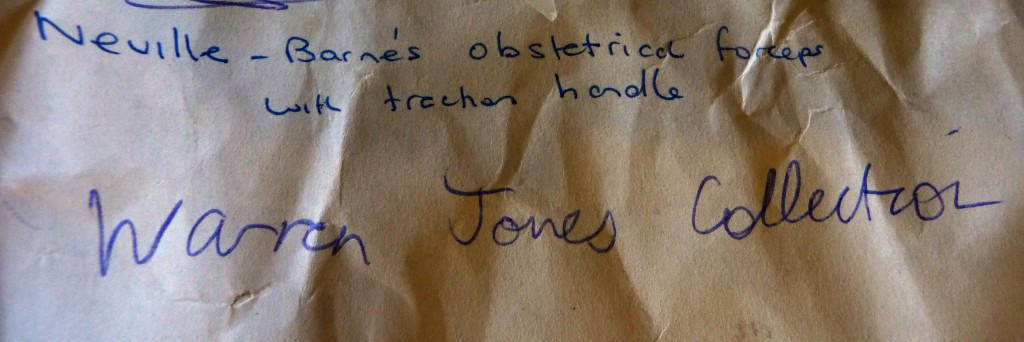
Emeritus Professor Warren Jones was the foundation Professor of Obstetrics at the Flinders Medical Centre. He donated his instruments to the Gus Fraenkel Library. The piece of paper above was in the box containing the forceps and identifies the type and name of the instrument, shown below. Separate parts (Lt.), assembled forceps (Rt.).


IN THE FIRST HALF OF THE LAST CENTURY, SURGEONS AND OBSTETRITIANS PROVIDED THEIR OWN INSTRUMENTS IN PRIVATE HOSPITALS WHICH WERE AUTOCLAVED BEFORE USE. DR COLIN SUCHTING KINDLY ALLOWED US TO PHOTOGRAPH THE FORCEPS HE USED. THEY ARE CONTAINED IN A METAL BOX. THE PERFORATED TRAY WAS PLACED IN THE AUTOCLAVE.
THE LID FROM DR. SUCHTING'S BOX INDICATING THE MANUFACTURER
THE FOLLOWNG PHOTOGRAPHS HAVE BEEN KINDLY PROVIDED BY BY THE GUS FRAENKEL LIBRARY AND ARE A PART OF PROFESSOR JONES' COLLECTION OF OBSTETRIC INSTRUMENTS.
THE SIMPSON PERFORATOR WAS USED TO DECREASE THE SIZE OF THE FOETAL HEAD OF THE STILL BORN BABY IN ORDER TO EASE THE DELIVERY AND TO SAVE THE MOTHER'S LIFE.
MILNE MURRAY FORCEPS FROM PROFESSOR WOODS COLLECTION.
PLEASE NOTE THE DIFFERENT BLADE SIZES AND A TRACTION HANDLE.

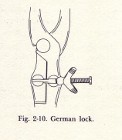
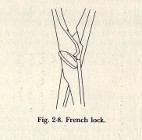
AS THE USE OF FORCEPS BECAME POPULAR, DESIGNERS INTRODUCED PERSONAL CHANGES WHICH INVOLVED MINOR DIFFERENCES IN THE PELVIC AND CEPHALIC CURVES, HANDLES AND LOCKING DEVICES.
THE ABOVE LOCKING DEVICES REPRESENT VARIOUS NATIONAL DESIGNS.
JAMES SIMPSON WAS A SCOTTISH OBSTETRICIAN WHO PRACTICED IN EDINBURGH IN THE 1850's.
HE WAS KEEN ON THE USE OF CHLOROFORM. HE OFTEN PLACED HIS INDEX FINGER BETWEEN THE HANDLES OR BLADES TO AVOID COMPRESSION OF THE FOETAL SKULL.
Assisted vaginal deliveries using forceps or vacuum devices has decreased markedly in recent times, and has been replaced by Caesarean section. The main reasons are possible damage to the foetus and/or the pelvic floor of the mother, and foetal haemorrhage which can be associated with vacuum extraction. The associated danger of litigation has also had a negative effect. In some countries the frequency of Caesarean section may exceed 30% of all deliveries. The Obstetric Colleges and other advisory bodies support a lower rate and there are attempts to improve training, education and appropriate accreditation for aspiring obstetritians.
-o0o-