South Australian Medical Heritage Society Inc
Website for the Virtual Museum
Home
Coming meetings
Past meetings
About the Society
Main Galleries
Medicine
Surgery
Anaesthesia
X-rays
Hospitals,other organisations
Individuals of note
Small Galleries
Ethnic medicine
- Aboriginal
- Chinese
- Mediterran
Bends, Caissons, Hyperbaric Oxygen, and the Adelaide Hyperbaric Unit
ACKNOWLEDGEMENT
We are most grateful to Tony Swain who reminded us of the early days of the Hyperbaric Oxygen Unit in Adelaide. We also thank Czes Mucha and Dr. David Wilkinson for allowing us a recent visit and providing the photographs. Greg Sampson provided the historical background; and Christy Pirone, a clinical nurse of the Hyperbaric Unit, published an article describing the early years in a RN Journal in 1990. We also thank Dr A. R. Laver and Professor Donald Simpson for their help and advice.
Bends
The word "bends" in the heading refers to the signs and symptoms which develop in persons who suffer decompression sickness. It is derived from 'the Grecian Bends' after a popular 19th century dance in which people bend at the waist. This condition can occur in divers who ascend too quickly from their dive (> 30m), or in aircraft which rise suddenly to high altitudes (> 20,000m). Thus aircraft are now pressurised.
The rapid decrease in pressure results in the release of absorbed nitrogen from the tissues, forming bubbles. This can cause the joints to become painful, and bending them helped reduce the pain. Hence a bent position.
Early Diving
People have been diving into water to collect resources (such as sponges, shells, pearls, salvaging shipwrecks, etc.) for several thousand years. As these divers were limited by their lung capacity, dives were relatively short and not very deep, and consequently decompression sickness would have been unlikely, and mild at worst.
Later advances included the use of rocks ("skandalopetra" in Greek). Both the diver and the stone were attached via a rope to a boat, allowing them both to be recovered faster. The diver jumped into the water holding the rock, sinking much faster with much less effort, increasing their productivity.
Diving bells have been used to work underwater for many centuries. Aristotle wrote about them around 400 BCE. They suffer many great disadvantages, e.g.: air was used up quickly, restricted to open water, and it must be lifted to extract resources and remove spoil.
Diving Suits
Early versions of diving suits are recorded from the 12th century, and possibly earlier. In 1405, Konrad Kyeser described a snorkel in his book "Bellifortis". Kyeser also described a metal helmet with two glass view-ports and a leather jacket, a forerunner of the standard diving dress. There are several other manuscripts from the 15th century with similar descriptions, including "Alte Armatur und Ringkunst" by Hans Talhoffer in 1459.
-
 A diver with a snorkel from Kyeser's Bellifortis.
A diver with a snorkel from Kyeser's Bellifortis. -
 A diving suit described by Talhoffer.
A diving suit described by Talhoffer.

The brothers Charles and John Deane designed the first successful diving helmets in the 1820's. They were originally intended to be used as smoke helmets by firemen, and used an external air supply. The helmets were made in 1827 by Augustus Siebe, and began to be used for diving around 1828. The helmets were loosely fixed to a diving suit, so divers could only work in an upright position without being flooded. Siebe later improved the suit, making it water tight, adding a valve in the helmet to stop water flooding in, and allowing the helmet to be removed from the corsetlet (the collar around the breastplate, back and shoulders that supports the helmet). The displacement of the suit would cause the diver to float, so additional weight had to be added, usually to the shoes and over the breastplate and helmet.

{kind=link}
The standard diving dress allowed for more mobility, kept the diver dry, and provided some protection from the cold. They did not protect the diver against decompression sickness or nitrogen narcosis.
Further improvements led to self contained underwater breathing apparatus (SCUBA). The two main types are closed-circuit and open-circuit. Closed-circuit cleans and recirculates the air, while open-circuit expels the air into the environment.
Closed-circuit re-breathers recirculate the air, chemically removing some of the carbon dioxide, and adding more oxygen from a tank. Giovanni Alfonso Borelli is credited with one of the earliest designs in the 17th century, but it was probably never tested. The first commercially successful model was designed by Henry Fleuss in 1878. Sir Robert Davis designed the first practical model made in large numbers in 1910.
The first commercially successful open-circuit SCUBA was the Aqualung, developed by Emile Gagnan and Jacques-Yves Cousteau in 1942-1943.
Both types of SCUBA divers can be affected by decompression sickness, depending on the depth, air mix and duration of the dive.
Bridges
Another way to access underwater sites (for building bridge piers, dams, etc.) is to construct a cofferdam. These are temporary, watertight enclosures, which allow workers to safely work on dry ground. While these give easy access, they are take up significant space, potentially interfering with trade routes, and are not well suited to deeper waters.
Caissons
One solution is to use caissons. Caissons are watertight containers which become part of the final structure. The word is derived from the French caisse, meaning "ammunition wagon", "crate", or "box". There are three main types: box, open, and compressed air.
Box Caissons
Box caissons are prefabricated boxes, often made of concrete, that are floated into position, before being sunk by being filled with concrete. Two different types of box caissons were used to build the Herodian harbour at Caesarea Maratime (about half way between the modern cities of Tel Aviv and Haifa, Israel) from 25 - 13 BCE. The harbour was built by order of Herod the Great, who named it Sebastos (Greek for "venerable", a translation of the Roman honorific augustus) and dedicated to the Roman Emperor Augustus. On the sheltered side, large hollow floating concrete boxes were towed into position, and then sunk by the addition of concrete. On the more exposed site, large seaworthy barges were used ( for more information, please refer to the Wikipedia article on Caesarea Maratima ).
Open Caissons
Open caissons are open topped, generally tube shaped walls which are sunk by their own weight, with a steel cutting shoe (a steeply angled leading edge) at the bottom. This technique was used by Marc Isambard Brunel in the construction of the access shafts to his Thames Tunnel in 1825 - 1843.
The Roman Emperor Trajan also used open caissons to build the piers for his bridge across the Danube, near the border of modern Serbia and Romania, in 103 - 105 CE. They used a wooden palisade wall, reinforced with metal bands, and lined with clay or pitch to excluded the water, and then drained. This allowed workers access to the river bed to build the foundations of the piers. The bridge was part of his supply route in the conquest of Dacia, and would have been a statement of Roman power. It remained the longest bridge (1,135m long, 15m wide, 19m high), and had the largest spans (38m) for more than a millennium.
Unpressurised caissons, such as that used in Brunel's Thames Tunnel do not cause decompression sickness. It wasn't until the 19th century that compressed air was used in caissons.
Pressurised Caissons
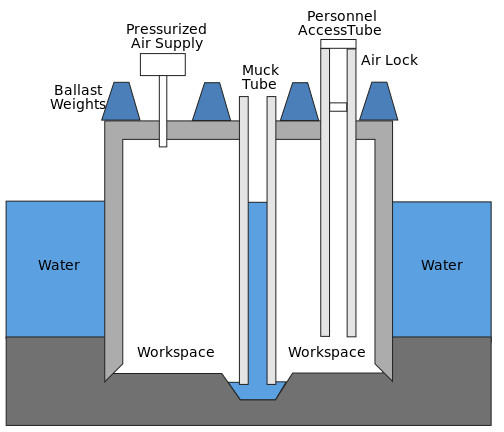
Compressed air caissons are essentially bottomless waterproof containers. Water is forced out by compressed air, providing a dry working environment. They have at least one airlock through which people can pass, compressed air shaft(s), and unpressurised shaft(s) allowing one or more cranes to extract the spoil (called muck). To reduce friction, the cutting shoe at the bottom is usually wider than the main body.
{kind=link}
Because they are less dense than the surrounding water, caissons need to be ballasted. This is usually achieved by the pier itself, although additional weight may be needed initially.
The deeper under water the caisson is, the more air pressure is needed, with every 10m of water adding one atmosphere of pressure. Excess air pressure escapes from under the bottom of the caisson, or via the muck tube. The air must be continuously supplied to replace the oxygen used by the workers, etc.
After the excavation has finished, the caisson is backfilled with concrete, becoming part of the final structure.
The modern version of the caisson was invented by the French geologist Jacques Triger in 1841. It consisted of 4 iron tubes, each approximately 1m wide, by 5-6m long, and most importantly, an airlock. This allowed him and others to mine coal at a depth of 20m in the water logged soil of the Loire river. Triger reported that two miners complained of pain after finishing working in 2.4 atmospheres for 4 hours, quite possibly the first recorded cases of decompression sickness (DCS).
As the amount of gas absorbed in water is proportional to the pressure (Henry's law), the greater pressures inside caissons causes more gas to be absorbed by the workers. As they return to the lower pressures outside, these dissolved gasses effervesce. If these bubbles form faster than they can be removed via the lungs, they can cause many problems, including skin rashes, joint pain, paralysis, emboli, and death, depending on their size and placement.
Decompression Sickness
One of the earliest description of decompression sickness was made in 1666 by the noted physicist and chemist, Robert Boyle (1627 - 1691). In his experiments with vacuums ("New Pneumatical Experiments about Respiration"), he noted "what I once observed in a viper furiously tortured in our exhausted receiver, namely, that it had manifestly a conspicuous bubble moving to and fro in the waterish humour of one of its eyes". He hypothesised that these bubbles could be dangerous. Felix Hoppe-Seyler demonstrated this experimentally in 1857 by the rapid decompression of various animals, finding considerable volumes of gas in the vena cava, and the right chambers of their hearts.
In 1847, the French doctors B. Pol and T. J. J. Watelle noted that recompression gave symptomatic relief to compressed air workers, and recommended a slow decompression to avoid further pain. They also noted a relation between symptoms and age, depth/pressure, duration of exposure, and decompression rate.
Another Frenchman, Dr Antoine Foley, recommended recompression as a treatment for DCS in 1863.
One of the earliest incidents of mass decompression sickness was recorded in during the construction of the Eads Bridge between St. Louis, Missouri and East St. Louis, Illinois across the Mississippi River in 1867. Caissons were sunk to reach the bedrock, the deepest was on the Illinois side, some 38m below the water level, requiring up to 55 psig (approx 4.7 atmospheres, car tyres are around 30 psig, or 3 atm). There were 119 severe cases, with 14 recorded deaths. The physician in charge, Dr Alphonse Jaminet, also suffered from decompression sickness and recorded his own description.
{kind=link}
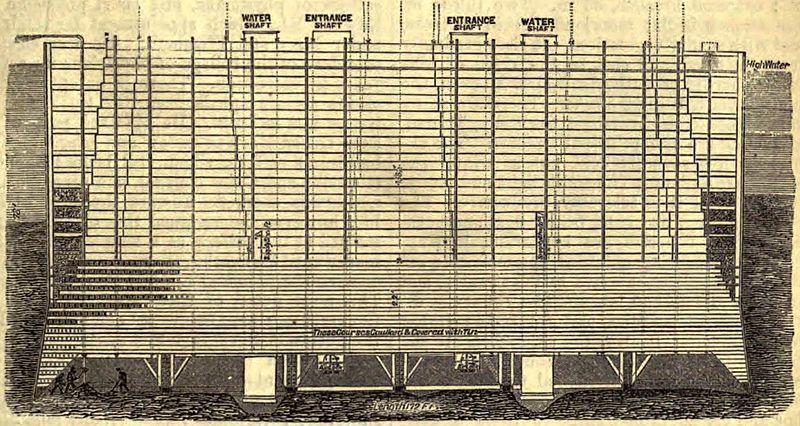
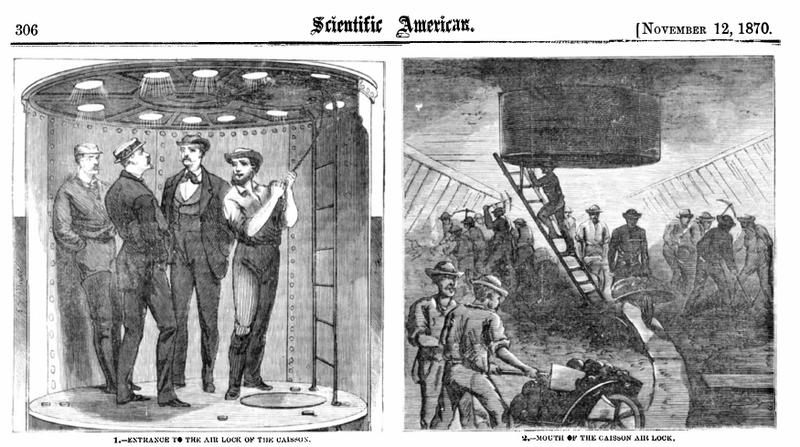
Perhaps the most famous use of caissons was the building of the Brooklyn bridge in 1871. In order to reach the bedrock under the East River (the deeper Manhattan side is about 24m below the waterline) a large wooden caisson was built on land, towed into the river, and sunk by building the pier on top of it. It was then filled with compressed air, allowing space for workers to excavate the ground below. After they had reached bedrock, the men left and the cavity was filled with concrete, becoming the foundation for the pier.
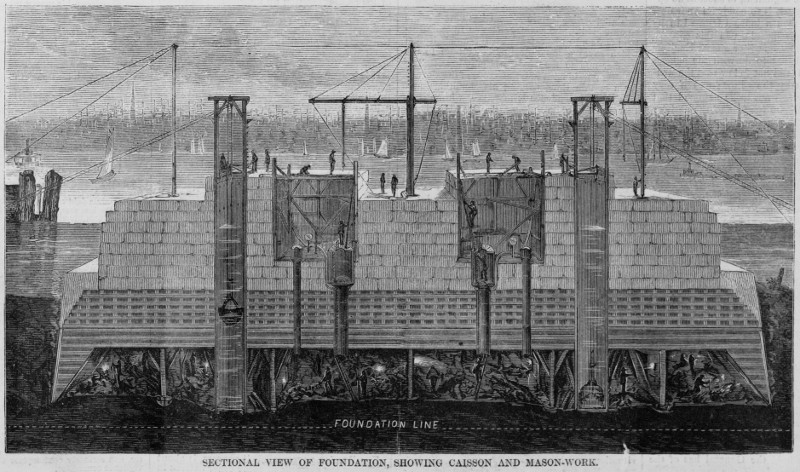
When the men had finished their shifts, they exited the caisson through a series of air locks. If they passed through too fast, they suffered from 'caisson disease', a term coined by the physician in charge of the project, Dr Andrew Smith, in 1873. He recorded 110 cases during construction, including 3 deaths. The project supervisor, Washington Roebling, also suffered from DCS in 1872, and was forced to oversee the last 10 year of construction from his house. He was greatly aided by his wife, Emily Warren Roebling, who nursed him, and trained herself as an engineer, taking over many of the duties of the chief engineer.
As a result of the deaths of these workers, both Smith and Jaminet made a series of changes to the working conditions, including:
- The number of hours of each shift was decreased based on the working pressures
- Compression locks, increasing by ~3 psi/min
- Longer post-work rest periods inside slowly decompressing rooms (~ 5-6 psi/min)
- Elevators were installed for the workers
- Fitness tests of workers, excluding
-
- the overweight
- older (>45-50 y.o.)
- those with heart or lung problems
- On-site hospitals
In 1872, Smith proposed the use of a medical lock (hyperbaric chamber), but it was never installed.
In 1878, the French physiologist Paul Bert showed that decompression sickness was caused by nitrogen gas being released from blood and tissue during or after decompression, much like what happens when a bottle of carbonated soft drink is opened. He also showed that DCS is more dangerous in the obese by repeatedly decompressing his dog, before fattening it up and trying again, resulting in its untimely demise. This was also noted by Smith and Jaminet, amongst others, in their recommendations after the bridge deaths.
It wasn't until 1889 that medical locks were used. After a British contractor took control of the first Hudson River Tunnel, Ernest William Moir installed a medical lock as described by Smith, reducing the death rate from 25% to 2%.
Decompression sickness is not limited to compressed air workers. The low pressures in mountaineering, unpressurised flight, and in space can also cause DCS. One example of this was the flight of the French balloon "Zénith" in 1875. Sponsored by Paul Bert and manned by Gaston Tissandier, Théodore Henri Sivel, and Joseph Crocé-Spinelli, the Zénith was launched to determine the composition of the upper atmosphere, reaching a height of approximately 8,600m. When they began to feel the effects of asphyxia, the men tried to reach their oxygen supplies, but were unable to as their arms were paralysed. Both Sivel and Crocé-Spinelli died, Tissandier survived, but became deaf.
Decompression Models
Early decompression models used uniform decompression rates. In 1895 the Austrian physiologist Hermann von Schrötter defined the safe decompression rate to be one atmosphere every 20 minutes. He also suggested using oxygen in recompression, but this did not become common due to fears of oxygen toxicity.
In 1901, after meteorologists in another balloon, the "Preussen" (German for "Prussia"), fell unconscious even with oxygen supplies, Schrötter realized that pressurised breathing equipment was needed in high altitudes to prevent hypoxia, proposing a pressurised sealed chambers for very high altitude flights.
Using goats as analogues for humans, the Scottish doctor John Scott Haldane developed a model for staged decompression rates, which took into account the depth, duration, nitrogen absorption and release rates in different tissues, and age of the diver. He proved that this was safer than the Schrötter's method of uniform decompression. From this model he produced his tables, presenting them to the British Admiralty in 1908, and were used until 1955. Together with A. E. Boycott and G. C. C. Damant, Haldane published the very influential paper "The Prevention of Compressed-air Illness" in the Journal of Hygiene, June, 1908.
The US Navy Experimental Diving unit also devised its own decompression tables. Their Air Decompression Tables from 1927 became a standard world wide.
From the 1960's, Albert A. Bühlmann, a Swiss physician, made several important refinements to Haldane's model, including dividing the tissues into more groups, and correcting for altitude. This lead to the development of the SAA (Sub-aqua Association) Bühlmann System in 1987. His ZHL-8 algorithm is used in many dive computers, and ZHL-16 algorithm is the basis for many tables.
In 1935, Albert R. Behnke et al. experimented with the use of oxygen in recompression therapy. They found it was effective, and it has become standard in the treatment of DCS. The reduced percentage of nitrogen in the hyperbaric oxygen air (and hence decreased nitrogen partial pressure), results in a greater partial pressure differential between the sufferer's blood and the breathed air. This increases the rate at which the nitrogen is removed from the patient, reducing the time required to safely decompress.
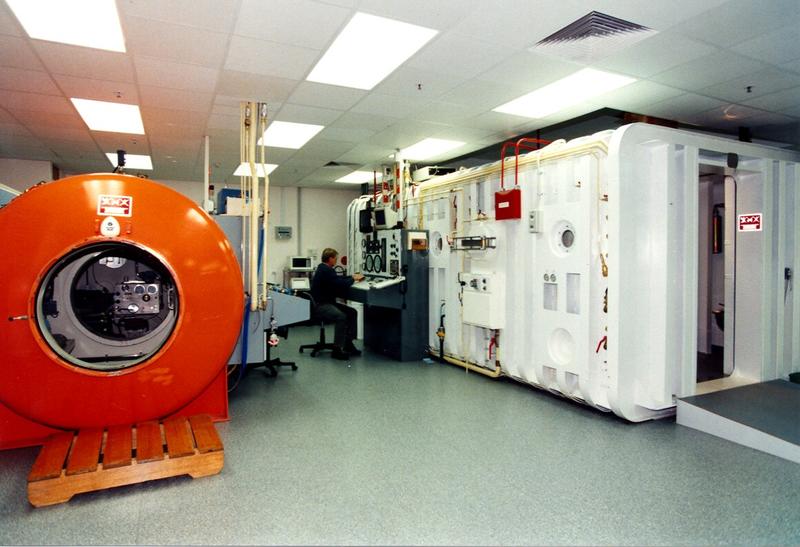
Adelaide Hyperbaric Unit
Before 1950, the need for decompression facilities in South Australia were relatively low, and any divers with decompression sickness were sent interstate in pressurised aircraft. There were however some individual attempts. Mr. McLaurie, a professional diver, constructed his own decompression chamber in the 1950's.
However new uses for hyperbaric oxygen were found. Several medical publications reported usage of the treatment in gas gangrene, necrotising fasciitis, carbon monoxide poisoning, trauma and other limb or cerebrovascular ischaemic episodes. It was thought to be of use in patients receiving radiotherapy and those with multiple sclerosis.
Another advance resulted from the discovery of the North Sea oil fields and the need for decompression treatment of several persons at the same time. This resulted in many technical innovations, and some of the superseded North Sea oil platform machines became available for other uses.
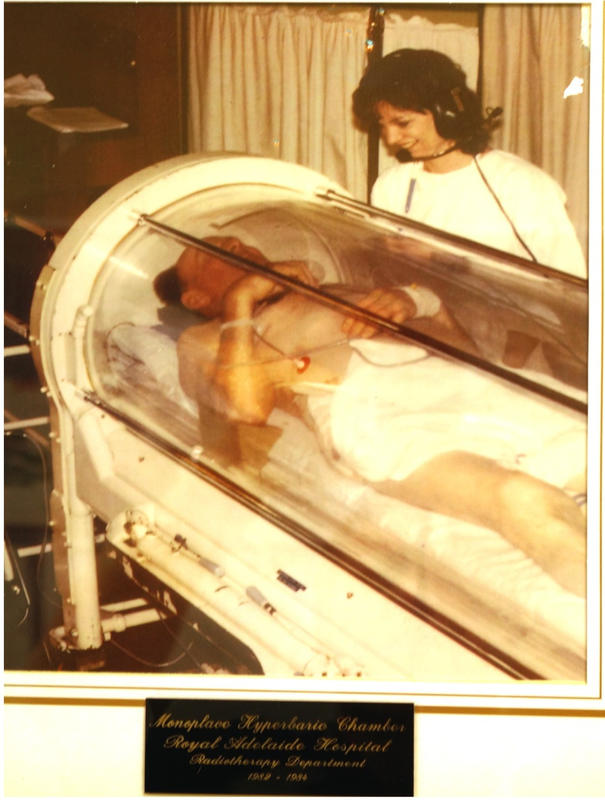
In Adelaide a single unit was used by the Radiotherapy Unit in early 1960. It was based on the belief that malignant cells were more susceptible to X-rays in a high oxygen environment. This type of therapy stopped with the arrival of better radiotherapy machines a few years later.
In 1982 Mr. Salkeld purchased a multiple marine decompression chamber from the Corshelf Marine company. It was sited in Kent Town (Adelaide), and was used in the treatment of multiple sclerosis. Several patients from the RAH with gas gangrene and caisson disease were also treated.
In the 1980's the need for a hyperbaric unit became obvious, and the Health Commission, State Government, and National Safety Council provided the stimulus and the finances. Drs. W. T. McCoy and J. E. Gilligan provided medical support.
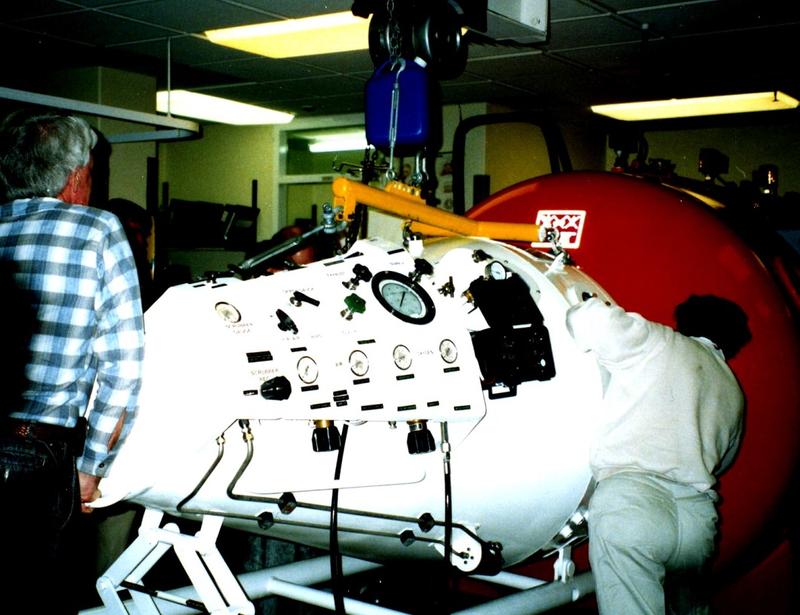
The first chamber, a single person unit, was purchased and installed in 1984. This was followed up by a square multi-chamber unit a year later. The Hyperbaric Oxygen Unit is still used, but its uses for decompression symptoms have decreased markedly. The current treatments are used on patients with acute or chronic wound problems, such diabetic ulcers, slow healing wounds, carbon monoxide poisoning, radiation cystitis and other post-radiation problems. Coupled with antibiotics, it is invaluable in treating gas gangrene and necrotising fasciitis. The case load is sufficiently large for the Unit to be opened each working day.
The Unit is located on Level 2 of the theatre bloc and, depending on the diagnosis, the treatment may need up to 40 attendances.
The following photographs and relevant comments show some of the history of the Unit.








From "Le Monde illustré", 1880.